
In our last blog we talked about the plank, squat and side plank. We will continue with taking a look at the single limb testing but before we do, we must look at three common motions we see at the hip during single limb testing.
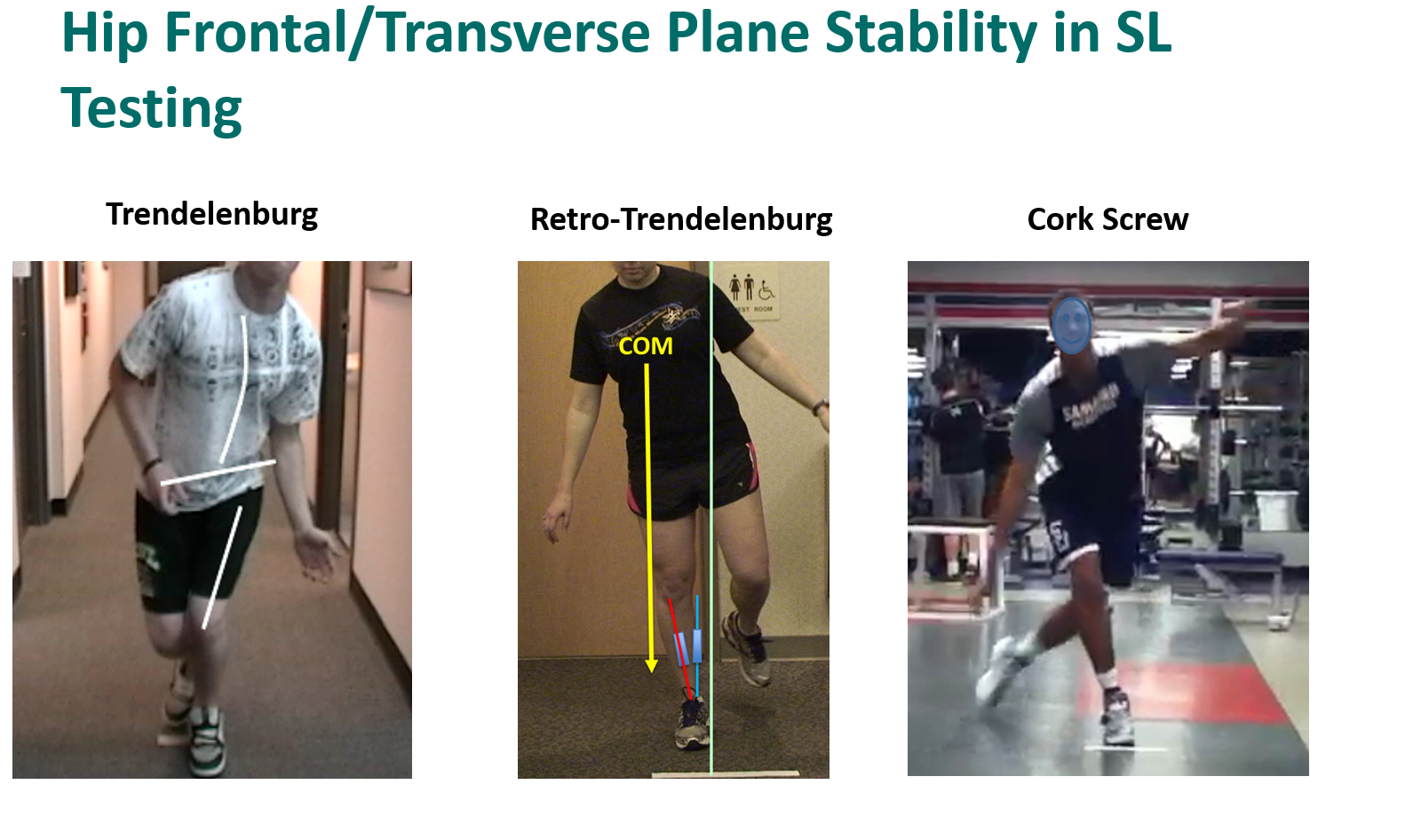
- Trendelenburg - in single limb stance, the contralateral hip (opposite hip - none stance leg) falls. This is indicative of gluteus medius weakness on the stance leg.
- Retro-trendelenburg - in this instance there is a little more weakness and the athlete subconsciously moves their center of mass (COM) laterally over the stance leg. This creates more acetabular coverage in the hip and hence is a more stable position at the hip and is a compensate for the weakness in the gluteus medius.
- Cork Screw - as the weakness progresses, the athlete is no longer able to stabilize the hip through multiple plans of motion. What happens is the athlete then falls into a trendelenburg with rotation. In this instance, the glutues medius is failing through its full range of motion.
With single limb testing, we start to see these motions at the hip become more obvious. It becomes even more obvious as we progress to hoping motion and hoping in multiple directions. When these motions become excessive, we often will see the athlete lose balance. In the test, this is recorded when the athlete touches down (with the leg they are holding up) or when they create stability by stabilizing against an external object (table, chair, etc).
We have also discussed the topic of "Time to Stability or TTS". This is the time it takes the athlete to stabilize after landing from a hop or multi-directional hop. We see this as the additional hops the athlete has once they land. We have seen and the research supports that the more hops they have to stabilize (or time), the more likely they are to get injured. What we see is that athletes who have a lack of pelvic stability (represented as a trendelenburg, retro-trendelenburg or cork screw) have much longer TTS than those who demonstrate the ability to stabilize their pelvis.
Since these motions are represented in all the single limb tests, it is important for us all to be able to identify them and put training in our programs that will correct.
Finally, prior to talking about each of the tests, we should also discuss the testing position. When testing single leg activities, we prefer the athlete to be in the "athletic" position. In this position, the knee is flexed to 45-90 degrees and the hip is in a neutral to slightly extended position (10-20 degrees). Not only is this more representative of a running position but also requires much more glut activity throughout the motion when compared to putting the hip in a flexed position or directly under the athlete. It is important that the athlete maintains this position (or attempts to) throughout the course of the test.
We have also discussed the topic of "Time to Stability or TTS". This is the time it takes the athlete to stabilize after landing from a hop or multi-directional hop. We see this as the additional hops the athlete has once they land. We have seen and the research supports that the more hops they have to stabilize (or time), the more likely they are to get injured. What we see is that athletes who have a lack of pelvic stability (represented as a trendelenburg, retro-trendelenburg or cork screw) have much longer TTS than those who demonstrate the ability to stabilize their pelvis.
Since these motions are represented in all the single limb tests, it is important for us all to be able to identify them and put training in our programs that will correct.
Finally, prior to talking about each of the tests, we should also discuss the testing position. When testing single leg activities, we prefer the athlete to be in the "athletic" position. In this position, the knee is flexed to 45-90 degrees and the hip is in a neutral to slightly extended position (10-20 degrees). Not only is this more representative of a running position but also requires much more glut activity throughout the motion when compared to putting the hip in a flexed position or directly under the athlete. It is important that the athlete maintains this position (or attempts to) throughout the course of the test.
 Single Leg Squat, Single Leg Hop, Single Leg Hop Plant - during this series of tests, we look for the ability to perform the test through an "expected range of motion" (range of motion is based on our normative data) while maintaining control of frontal plane motion (both how much the knee moves and the speed at which it moves). Total frontal plane motion (varus to valgus) should be = to or < 10 degrees and valgus speed is dependent on the movement that is being performed (defined below).
Single Leg Squat, Single Leg Hop, Single Leg Hop Plant - during this series of tests, we look for the ability to perform the test through an "expected range of motion" (range of motion is based on our normative data) while maintaining control of frontal plane motion (both how much the knee moves and the speed at which it moves). Total frontal plane motion (varus to valgus) should be = to or < 10 degrees and valgus speed is dependent on the movement that is being performed (defined below). Movements Assessed:
- Frontal plane motion - ideally the total frontal plane motion should be 10⁰ or less. Motion >10⁰ puts excessive stress on the tissues and structures of the knee, hip and spine. Controlling this motion is primarily provided by the gluteus maximus and gluteus medius. There are other weaknesses that can drive this motion (excessive foot pronation) but in the majority of cases this is driven by the weakness in the hip. In addition, poor core stabilization (excessive motion of the center of mass), and also result in excessive frontal plane motion of the knee.
- Speed of motion - the speed at which the knee falls into a valgus motion has a greater impact on stress imparted to the tissues and structures of the knee than motion alone. As the loads or demands increase, it is even more important to control these motions. For example, the loads for single leg squat are less than single leg hop which is less than single leg hop plant. Speeds should be:
- Single leg squat - speed should be equal to or less than 20 degrees per second
- Single leg hop - speed should be equal to or less than 100 degrees per second
- Single leg hop plant - speed should be equal to or less than 135 degrees per second
Controlling of excessive speeds requires training in three areas:
- Core control - controlling the center of mass during single leg activities
- Gluteus medius and maximus strength and endurance
- Rapid neuromuscular response - creating exercises which require a rapid neuromuscular response is what is needed to maintain stability in high velocity and under high load demands
As you can see, specific isolated movements within each of the tested positions can guide us on much more targeted interventions. We hope you enjoyed this series. If you did, please share with your colleague and follow us on instagrm @ bjjpt_acl_guy and twitter @acl_prevention. #ViPerformAMI #ACLPlayItSafe
Dr. Nessler is a practicing physical therapist with over 20 years sports medicine clinical experience and a nationally recognized expert in the area of athletic movement assessment and ACL injury prevention. He is the founder | developer of the ViPerform AMI, the ACL Play It Safe Program, Run Safe Program and author of a college textbook on this subject. Trent has performed >5000 athletic movement assessments in the US and abroad. He serves as the National Director of Sports Medicine Innovation for Select Medical, is Vice Chairman of Medical Services for USA Obstacle Racing and movement consultant for numerous colleges and professional teams. Trent has also been training and a competitive athlete in Brazilian Jiu Jitsu for 5 years.
No comments:
Post a Comment