
Hop Distance Symmetry Does Not Indicate Normal Landing Biomechanics in Adolescent Athletes with Recent Anterior Cruciate Ligament Reconstruction.

The following conclusions came out of this study. Both symmetric and asymmetric patients offloaded the operative knee and symmetric patients achieved symmetry in part by hopping a shorter distance on the contralateral side. Therefore, hop distance symmetry may not be an adequate test of single limb function and return to sport readiness.

The other result, symmetric patients achieved symmetry in part by hopping a shorter distance on the contralateral side. This test is designed to be a way to assess limb symmetry index or the variance between the right side and the left side. Studies have shown (Rhoman et al Am J Sports Med 2015) that norms have a limb symmetry index of 85%. Considering this, it is hypothesized if an athlete has a variance >15% on the right versus the left, then they are at greater risk of injury. Based on the results here, we can make the assumption that this test will not show us who is at risk. Whether consciously or unconsciously, the athlete is modifying effort on the non-involved limb which will misrepresent the true limb symmetry index.
However, the area of biggest focus for most of us is what are the biomechanics at take-off and landing? As the athlete is going into loading the limb for explosive power and begins to explode up, it is usually the transition from loading the limb to explosive movement that you will see the knee move into the dynamic valgus position. This is a focus for most as we know that this motion is the one that will or could potentially lead to increase risk for ACL injury or mensical injury.
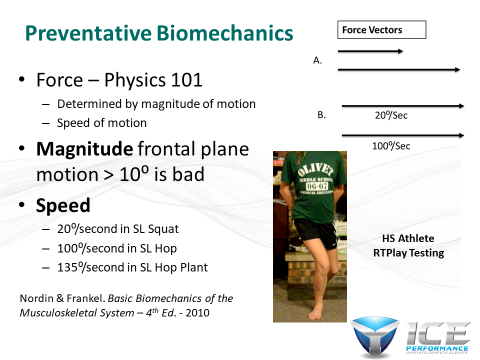
If you take the above slide as an example, you will see that based on basic biomechanics that force is determined by both the magnitude of the motion (how much the knee moves into valgus) and speed (how fast it moves into valgus) at which that motion occurs. So the larger the valgus is at loading and the faster that valgus occurs at loading, the greater the risk is that force will be departed to the ACL and the meniscus. This is something we want to measure and quantify. According to Johnston et al Am J Sports Med 2018, based on video review of non-contact ACL injuries in football players, dynamic valgus is the position that causes ACL rupture which led the authors to suggest this should be something that is assessed to identify those at risk.
This same motion is typically observed again at landing. When the athlete’s foot contacts the ground and they have to being to attenuate the force through the foot/ankle, knee and hip. It is typically at this point under high loads that you will again observe the knee move into the dynamic valgus position. Considering the ground reaction forces generated in landing (on a basketball court) is anywhere from 4-8 times body weight, we can understand the importance of controlling this motion during these movements.
This study also showed there was lower knee flexion moments and subsequent decrease in energy attenuation along the system. We see this a lot in athletes following an ACLR and think a lot of this has to do with mental compensation and lack of training.
First let’s look at mental compensation leading to lower knee flexion moments. What we suspect in these cases is the athlete subconsciously knows they lack the control of the knee to prevent dynamic valgus at larger knee flexion angles. This is a position that gives them a lot of fear (kinesiophobia - fear of movement) since they subconsciously know this is the position during which they tore their ACL. As a result of the fear, they will subconsciously compensate and not allow themselves to fall into larger knee flexion angles because they loose control. If they allow greater flexion angles during the landing phase then they will fall into this dynamic valgus motion and potentially rupture their ACL. If this is not addressed (through out their rehab and return to play) then this adds to greater ground reaction forces being distributed to the knee, hip and low back. This will break down tissue and potentially result in additional non-contact injuries. In addition to this, it can also add to a lack of force production. Most will demonstrate both in landing and take-off. In take-off, by decreasing flexion angles, this results in a decrease in force production and power output.
Next week, we will look at the lack of training and how this leads to decreased knee flexion angles. Please make sure to check out our new website at www.iceperform.com where our goal is to help you help others. #ViPerformAMI
Dr. Nessler is a practicing physical therapist with over 20 years sports medicine clinical experience and a nationally recognized expert in the area of athletic movement assessment. He is the founder | developer of the ViPerform AMI, the ACL Play It Safe Program, Run Safe Program and author of a college textbook on this subject. Trent has performed >5000 athletic movement assessments in the US and abroad. He serves as the National Director of Sports Medicine Innovation for Select Medical, is Vice Chairman of Medical Services for USA Obstacle Racing and movement consultant for numerous colleges and professional teams. Trent is also a competitive athlete in Brazilian Jiu Jitsu.
No comments:
Post a Comment